Devices and methods for performing a vascular anastomosis
a technology of vascular anastomosis and devices, which is applied in the field of devices and methods for performing vascular anastomosis, can solve the problems of not always achieving a leak-free seal, requiring much skill and practice on the part, and time-consuming and difficult task of suturing the anastomose, so as to reduce the amount of manual manipulation necessary, improve the anastomosis procedure, and the effect of rapid, efficient and reliabl
- Summary
- Abstract
- Description
- Claims
- Application Information
AI Technical Summary
Benefits of technology
Problems solved by technology
Method used
Image


Examples
first embodiment
[0084]FIG. 1 is a perspective drawing of the anastomosis staple device of a first aspect of the present invention. The anastomosis staple device 100 consists of two parts: an anchor member 101, and a coupling member 102. The anchor member 101 forms the attachment to the exterior surface of the wall of a target vessel such as the aorta. The coupling member 102 forms the attachment to the bypass graft vessel. When the coupling member is joined to the anchor member, as shown by the dotted lines 103, it forms a complete anastomosis.
[0085] The anchor member 101 has a ring-shaped frame 104 which is configured to encircle an opening in the wall of a target vessel, such as the aorta. The ring-shaped frame 104 has a plurality of attachment legs 105, preferably six to twelve, circumferentially spaced around the frame 104 and projecting from the distal end 106 of the ring. The anchor member 101 is preferably made of stainless steel or a titanium alloy for strength, biocompatibility and absence...
second embodiment
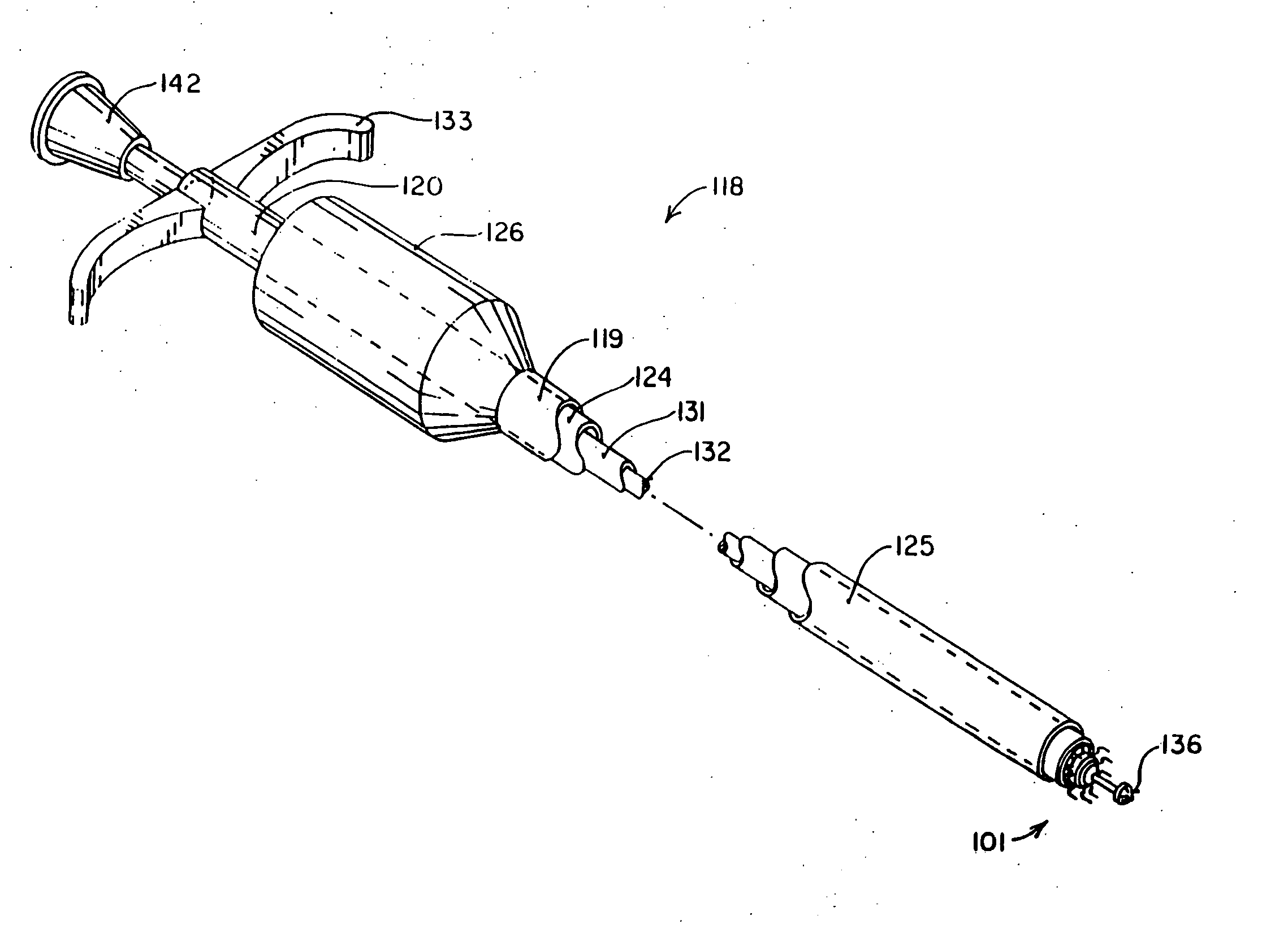
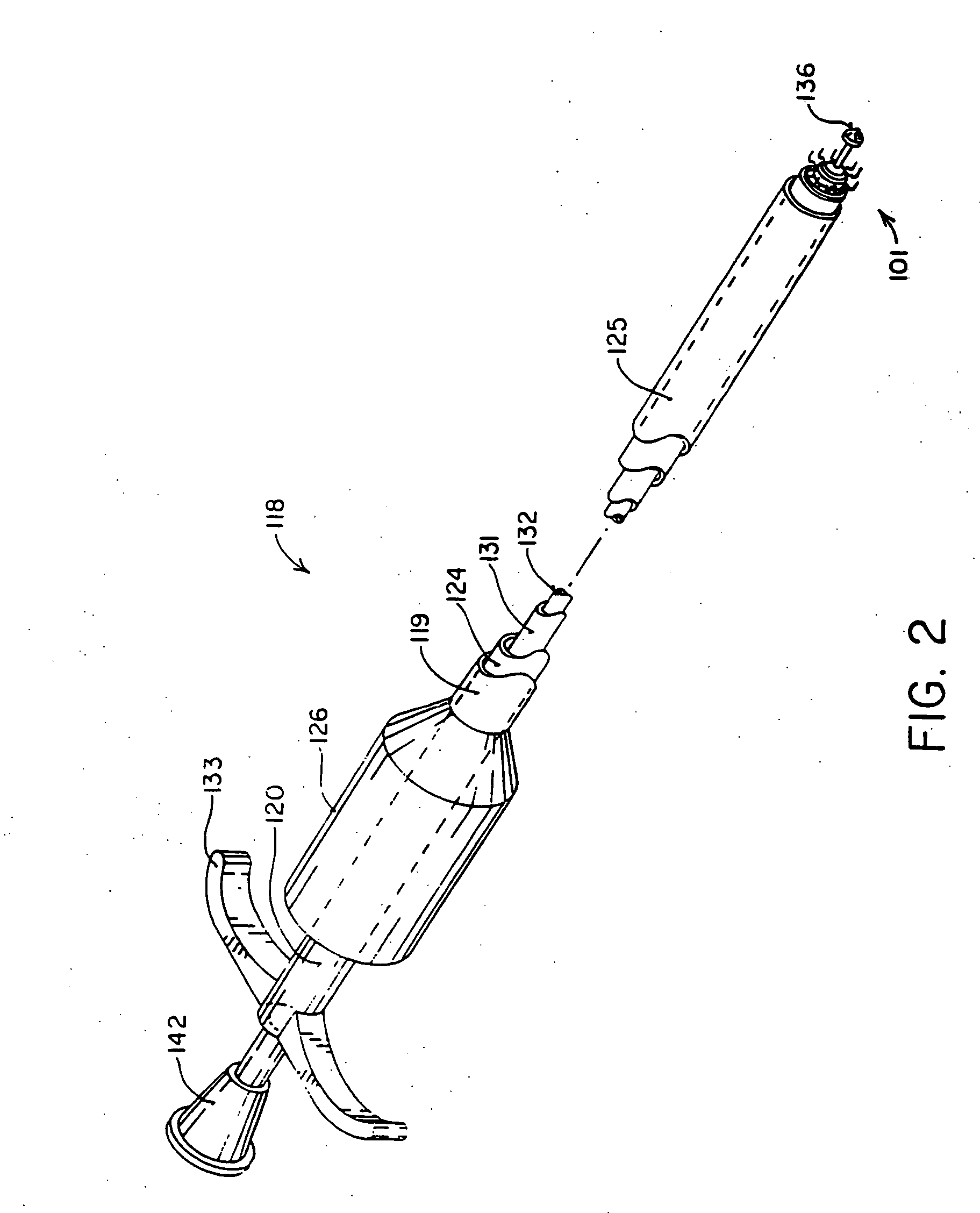
[0103]FIG. 7A shows a perspective drawing of the graft insertion tool 122 for use in performing the second anastomosis on a graft vessel, one end of which has already been anastomosed, or for other situations when both ends of the graft vessel are not available, such as when making the distal anastomosis on an internal mammary artery bypass graft. This embodiment of the graft insertion tool 122 is made with a two-part, hinged holder 154 for the coupling member of the anastomosis staple device so that the holder 154 can be removed from around the graft vessel 148 after both ends of the graft have been anastomosed. The holder 154 is attached to the distal end of a tubular member 155 which is attached on its proximal end to a handle grip 156. A shaft 157 is slidably received within the tubular member 156. The distal end of the shaft 157 is attached to a U-shaped yoke 158 which is configured to grip a flange 159 or a pair of lugs on the proximal end of the anchor member 101. The handle ...
PUM
 Login to View More
Login to View More Abstract
Description
Claims
Application Information
 Login to View More
Login to View More - R&D
- Intellectual Property
- Life Sciences
- Materials
- Tech Scout
- Unparalleled Data Quality
- Higher Quality Content
- 60% Fewer Hallucinations
Browse by: Latest US Patents, China's latest patents, Technical Efficacy Thesaurus, Application Domain, Technology Topic, Popular Technical Reports.
© 2025 PatSnap. All rights reserved.Legal|Privacy policy|Modern Slavery Act Transparency Statement|Sitemap|About US| Contact US: help@patsnap.com