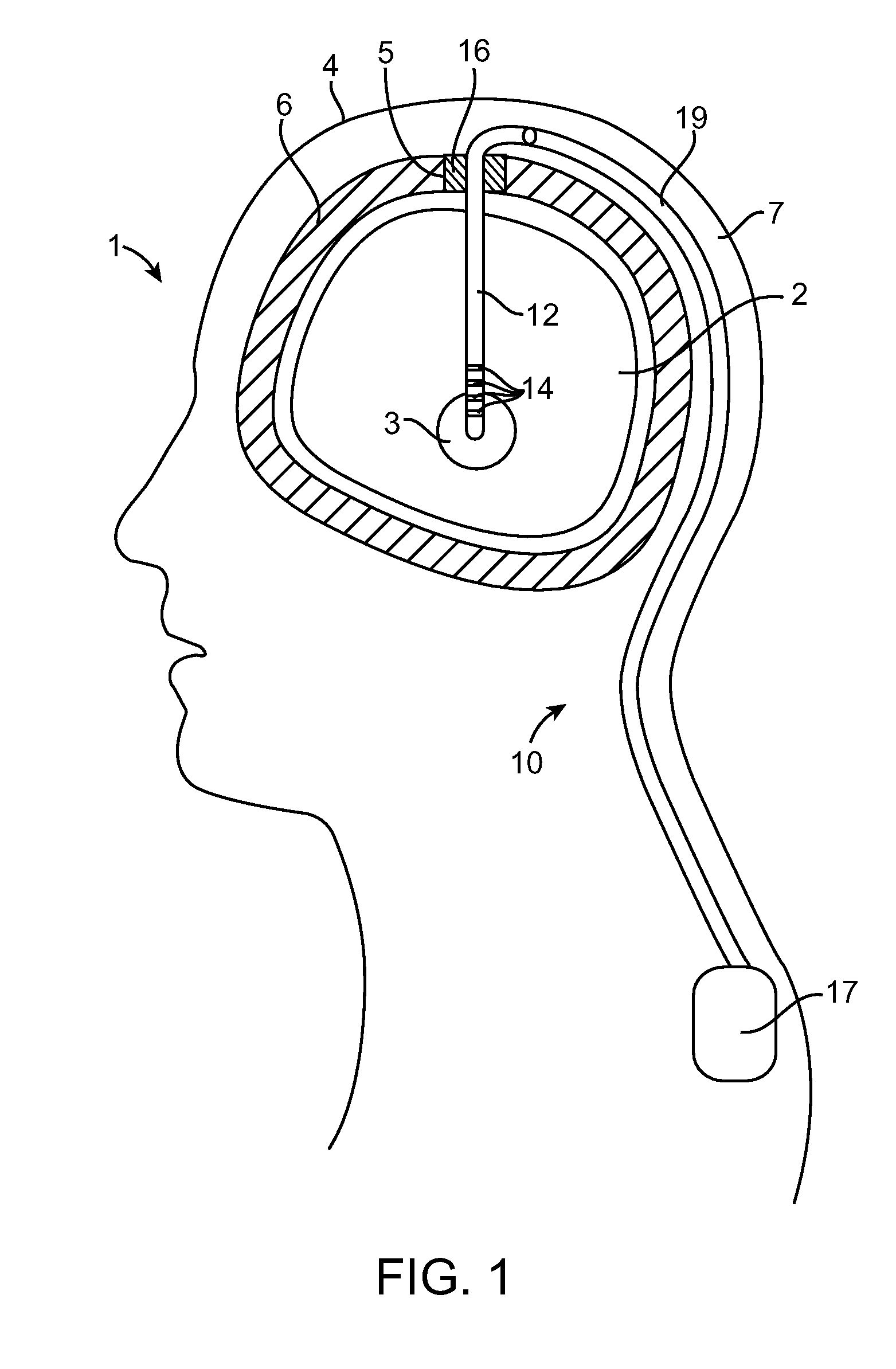
Thus, lead displacements of less than a
millimeter may have a deleterious effect on the patient's therapy.
Notably, any displacement of the portion of the lead exiting the burr hole will result in the translation of the electrodes positioned in the brain relative to the
target site, thereby requiring the lead to be repositioned—a time-consuming process.
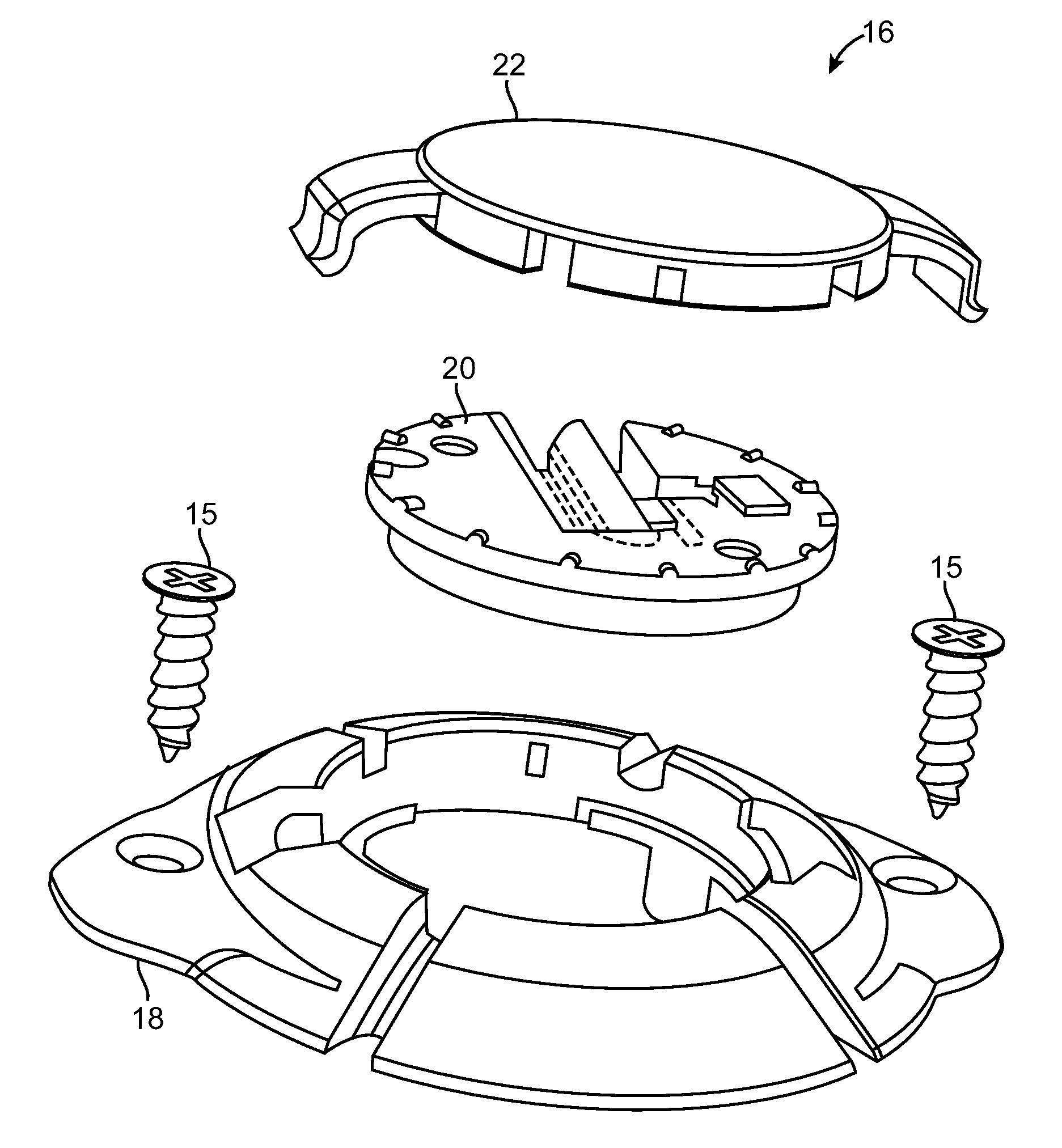
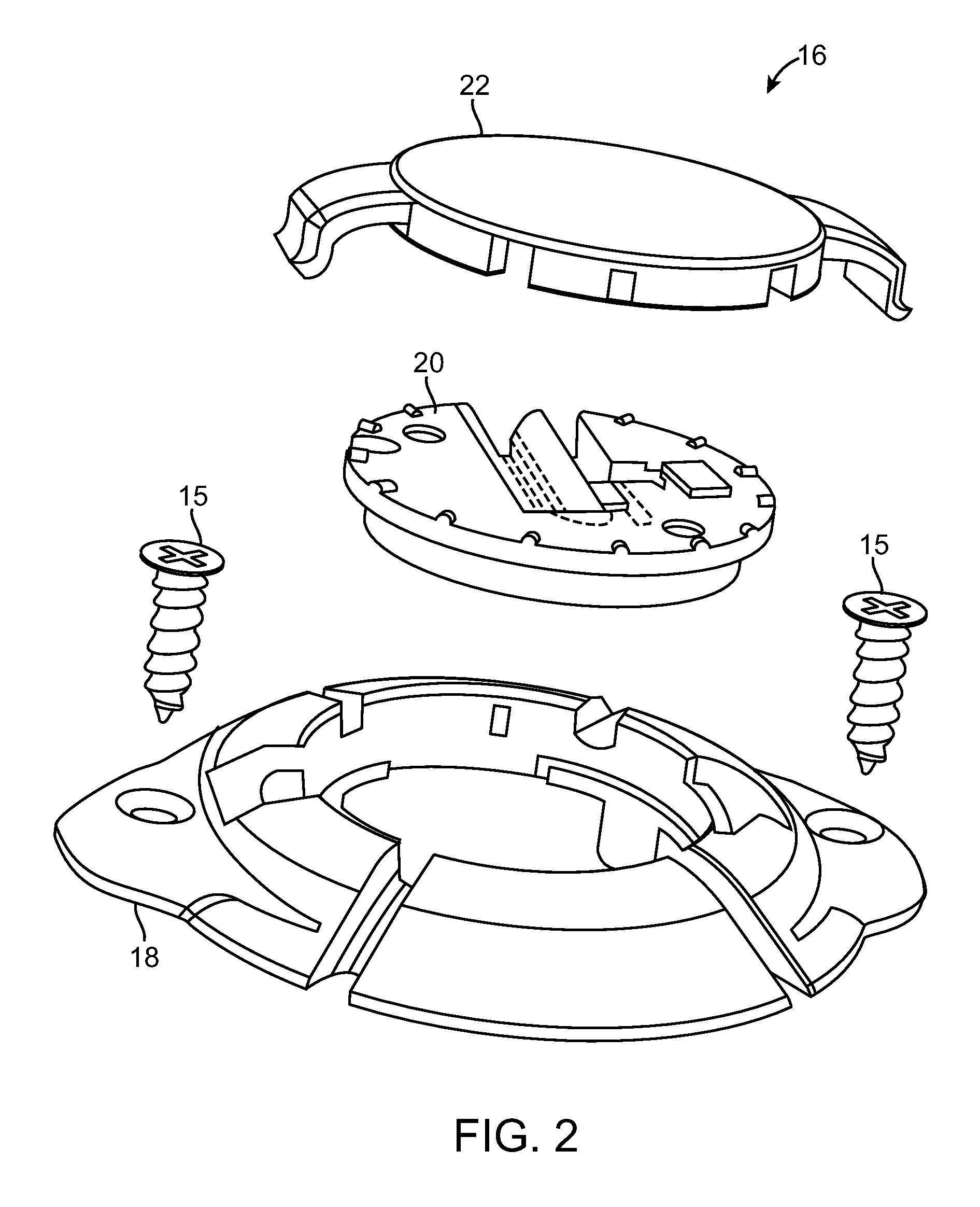
Also, because prior art plug bases are composed of a single piece, there is a risk that the plug base may fracture if the plug base is anchored to tightly to the cranium of the patient, especially if the bottom surface of the plug base does not match the curvature of the cranium.
In addition, because the clamping mechanism will deform somewhat along its length when clamped against the stimulation lead, an unequal force may be applied along the clamping mechanism, thereby weakening the retention force applied to the lead.
Also, because of the relatively weak composition of the retainer, the clamping force between it and the
mating surface of the disk is limited, thereby limiting the lead retention force of the clamping mechanism.
Furthermore, because the application of a downward force is typically necessary to unlock and allow the clamping mechanism to rotate relative to the disk, such downward force may cause the clamping mechanism to be bent too far down, thereby permanently deforming or breaking it.
In addition, since burr hole plugs are typically composed of
biocompatible polymers that are extremely lubricious, particularly when wetted, the
coefficient of friction of the retention surface of the clamping mechanism, as well as the
mating surface of the disk, may be relatively low.
As another example of a problem suffered from prior art burr hole plugs, the retainer may rotate within the plug base, potentially resulting in the inadvertent movement of the stimulation lead from the
target site.
However, prior art burr hole plugs are not designed to stabilize more than one stimulation lead at time.
By creating multiple
burr holes, the risk to the patient, time in the operating room (which also increases
patient risk), the materials and staff needed in the operating room, and cost of the procedure are all increased, so a burr hole plug that can accommodate multiple leads through one burr hole is preferred.
However, because the recess of the plug base in which the lead is seated may be located obliquely (as opposed to perpendicular) to the slot, it may be difficult to bend the lead perpendicular to the slot towards the base recess if the lead support mechanism is not perfectly oriented relative to the plug base.
In addition, rotation of the lead support mechanism relative to the base while the lead is seated within the base recess may cause the lead to be displaced from the
target site.
However, due to the diminutive size of the burr hole plug components, they are difficult to position, manipulate, and
handle.
This, in combination with the limited
working space between the targeting apparatus and the burr hole, makes it quite difficult to visualize and correctly install the plug within the burr hole and stabilize the lead.
While the surgeon is installing the components of the burr hole plug, there is a risk of foreign objects (screws, tools, debris, etc.) falling into the exposed burr hole, as well as slippage of tools within the burr hole.
However, the screws often pop-out of these tools unintentionally and do not always screw into the cranium at the correct angle.
Thus, installation of the burr hole plug without disturbing the lead position is nearly an impossible task without specialization of the tools and / or burr hole plug that can center the plug base while it is anchored to the patient's
skull and securely hold and
mount the retainer to the plug base.
However, this installation tool only engages the retaining disk at one location.
Thus, it is possible that the disk may become skewed or tilted while attempting to install it within the plug base, or worse yet, given the
spring force stored in the disk, it may be launched from the
surgical site.
If the
diameter of the actual lead used with the burr hole plug is smaller than this intended, the retention force applied to the lead by the clamping mechanism will not be sufficient.
If the
diameter of the actual lead used with the burr hole plug is greater than this intended
diameter, too much force will need to be applied to the lead in order to place the clamping mechanism within the locking position, thereby potentially damaging the retainer and / or the lead.
As yet another example, once the plug base is mounted to the patient's cranium via screws, it is difficult to adjust the position of the plug base if it is desired.
Also, due to the relatively
large size of the stereotactic targeting apparatus, there is often little
working space available between the targeting apparatus and the burr hole to anchor the plug base to the cranium of the patient.

 Login to View More
Login to View More  Login to View More
Login to View More