External fixation and foot-supporting device
a technology of external fixation and support device, which is applied in the field of therapeutic orthopedic devices, can solve the problems of long treatment duration, cumbersome external fixation structure, patient's foot and lower leg immobilization, etc., and achieve the effects of reducing complexity, reducing pain, and normalizing gai
- Summary
- Abstract
- Description
- Claims
- Application Information
AI Technical Summary
Benefits of technology
Problems solved by technology
Method used
Image

Examples
Embodiment Construction
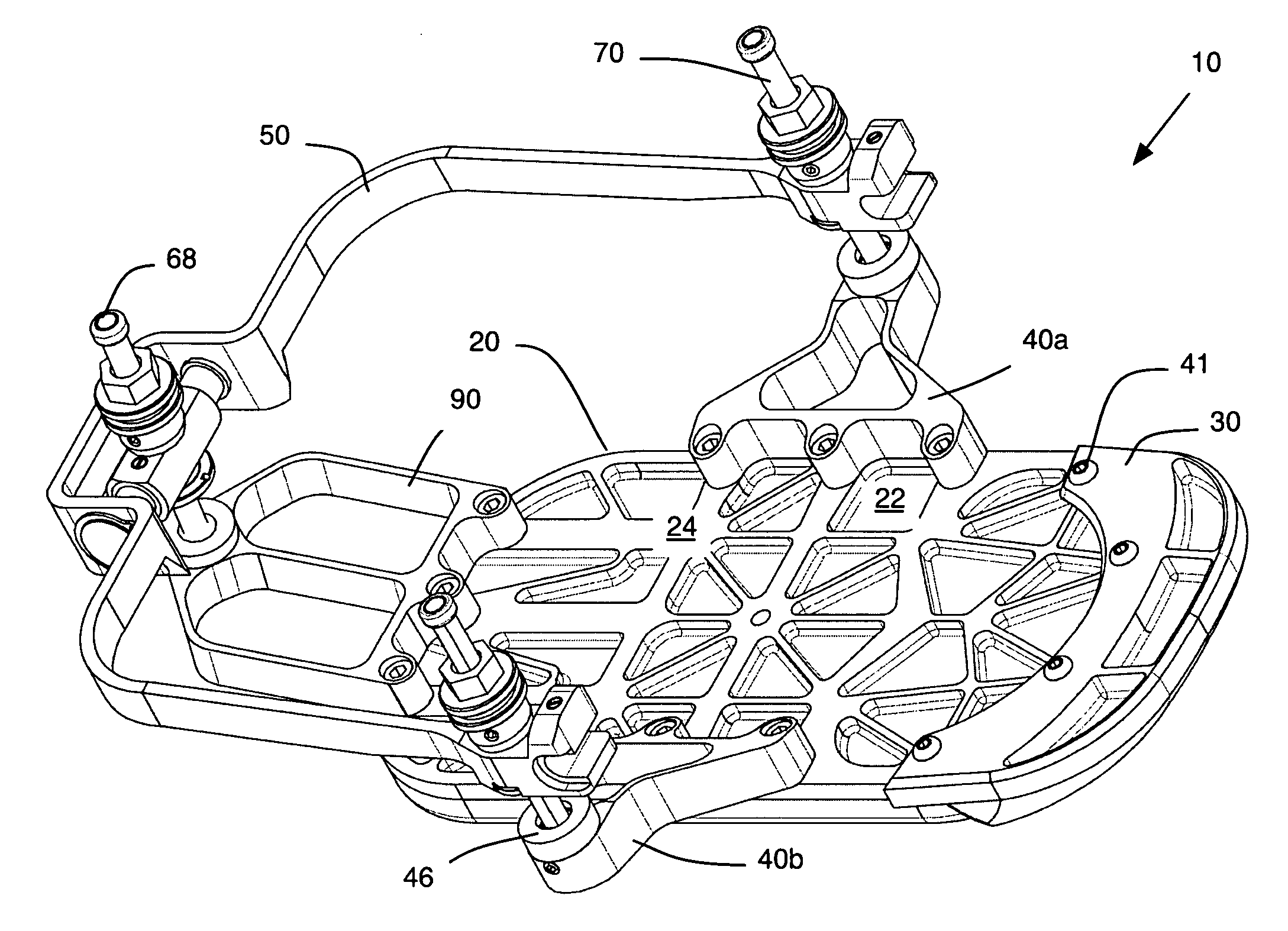
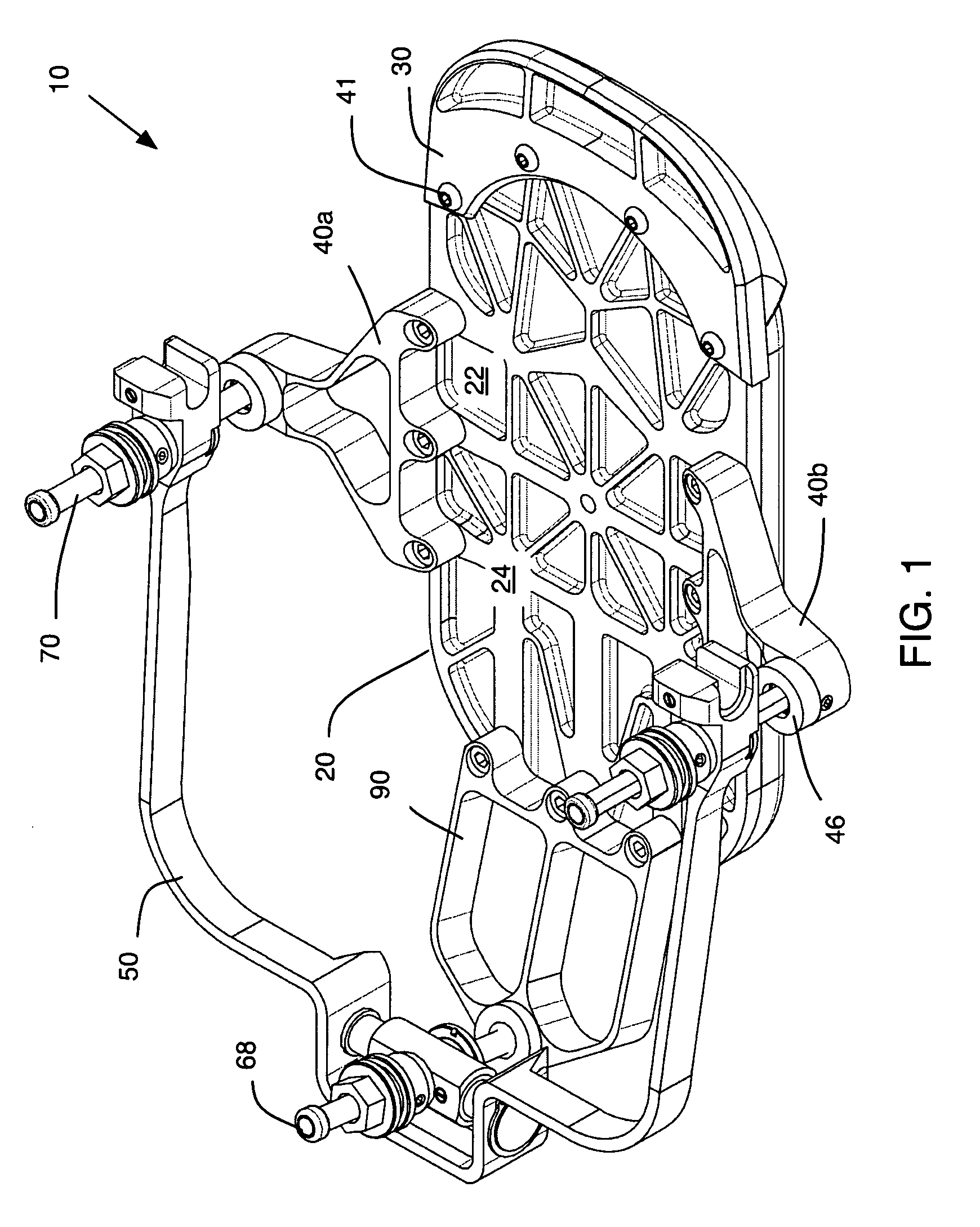
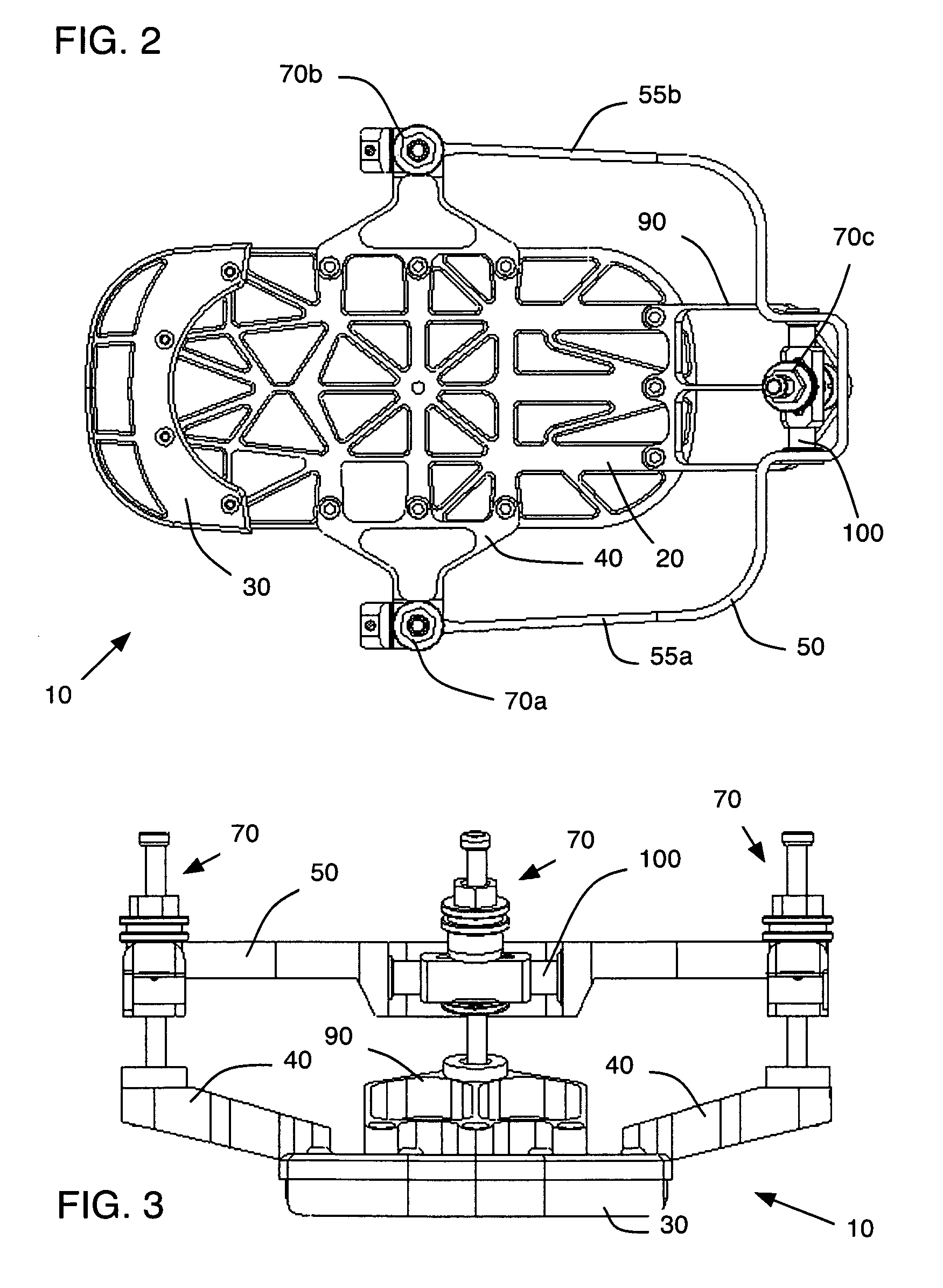
[0077]Possible embodiments will now be described with reference to the drawings and those skilled in the art will understand that alternative configurations and combinations of components may be substituted without subtracting from the invention. Also, in some figures certain components are omitted to more clearly illustrate the invention. In the prior-art, the term “foot-ring” and “foot-plate” often are used synonymously. However, in the present invention an attempt is made to distinguish the known prior art device that surrounds the foot (foot ring) from the present invention that includes components that couple to this foot ring and components adapted for use by the plantar surface of the foot. The later type components are termed foot-plates, or as used herein, a base plate.
[0078]FIGS. 1-4 illustrate a first preferred embodiment of the present invention and provide an overview contextualizing the various components. In this embodiment, a FRAMEWALKER™ brand (available from Quantu...
PUM
 Login to View More
Login to View More Abstract
Description
Claims
Application Information
 Login to View More
Login to View More - R&D
- Intellectual Property
- Life Sciences
- Materials
- Tech Scout
- Unparalleled Data Quality
- Higher Quality Content
- 60% Fewer Hallucinations
Browse by: Latest US Patents, China's latest patents, Technical Efficacy Thesaurus, Application Domain, Technology Topic, Popular Technical Reports.
© 2025 PatSnap. All rights reserved.Legal|Privacy policy|Modern Slavery Act Transparency Statement|Sitemap|About US| Contact US: help@patsnap.com