Biological navigation device
a technology for biological navigation and luminal cavities, applied in medical science, surgery, diagnostics, etc., can solve the problems of high part count, high cost of a lower cost, patient danger, etc., and achieve the effect of reducing creasing and high packing density
- Summary
- Abstract
- Description
- Claims
- Application Information
AI Technical Summary
Benefits of technology
Problems solved by technology
Method used
Image

Examples
Embodiment Construction
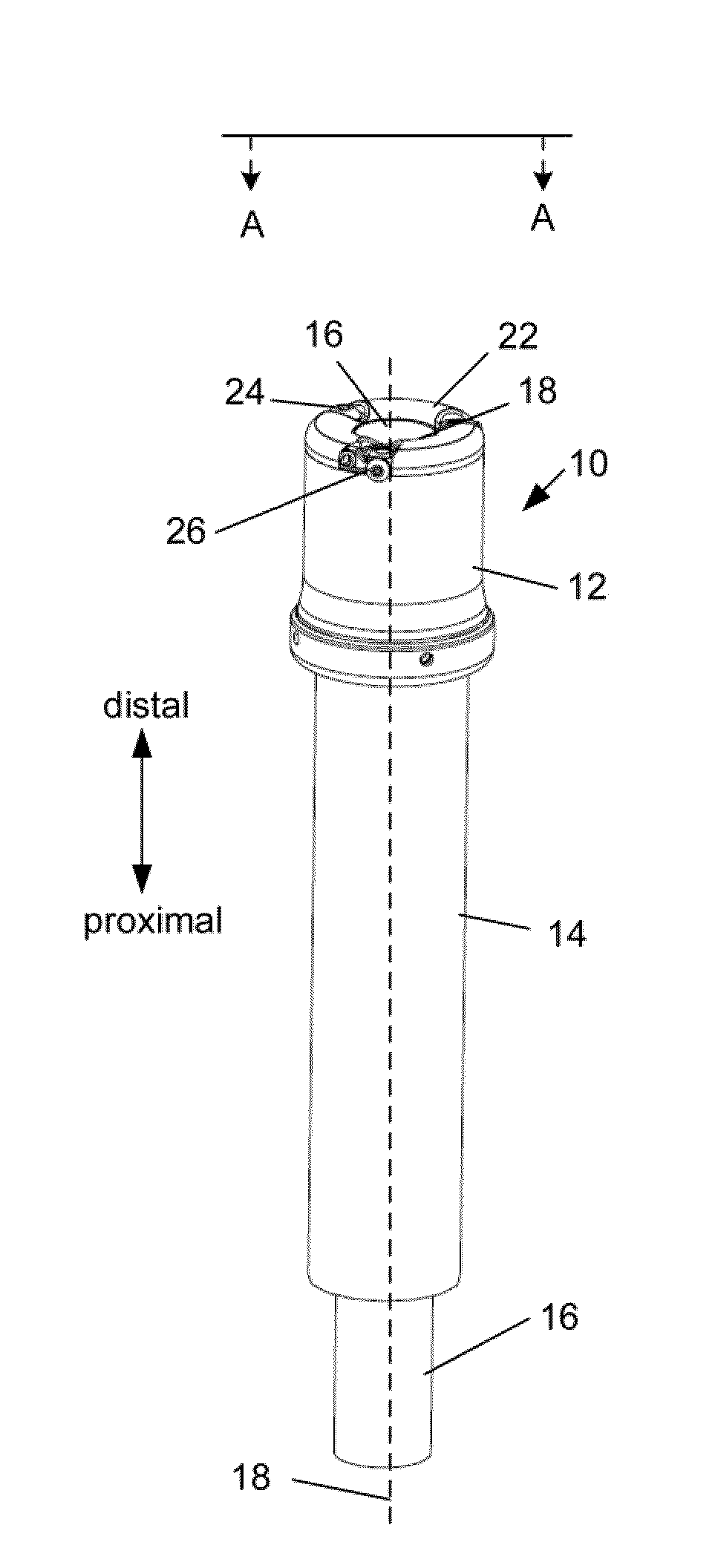
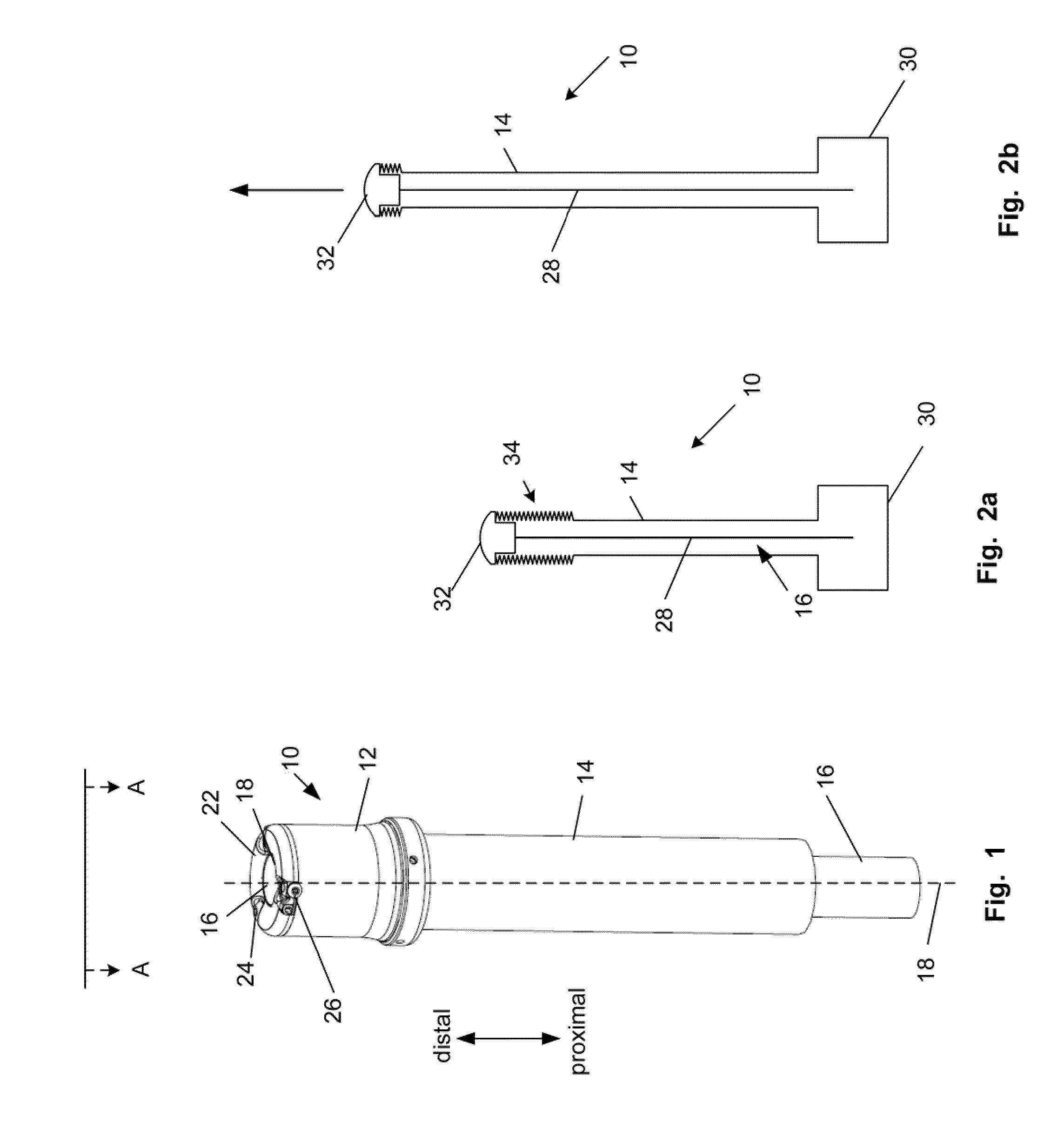
[0111]FIG. 1 illustrates a biological navigation device 10. The device can be used for navigation through a biological anatomy, such as a biological lumen, for example any or all of the GI tract (e.g., colon, stomach, esophagus) or cardiovascular vessels (e.g., arteries, veins, heart chambers).
[0112]The navigation device can be removably attached or integrated (e.g., permanently fixed, welded, glued, fused, or otherwise substantially permanently fixed) with an elongated element. The elongated element can be, for example, an endoscope or colonoscope. For example, the elongated element can be a CF-Q160 series, PCF-160 series, or CF-2T160 series colonoscope (from Olympus America, Inc., Center Valley, Pa.), a Pentax EC-series colonoscope (from Pentax of America, Inc., Montvale, N.J.), a Fujinon HD Super CCD colonoscope, or a G-5 endoscope (from Fujinon Inc., Wayne, N.J.).
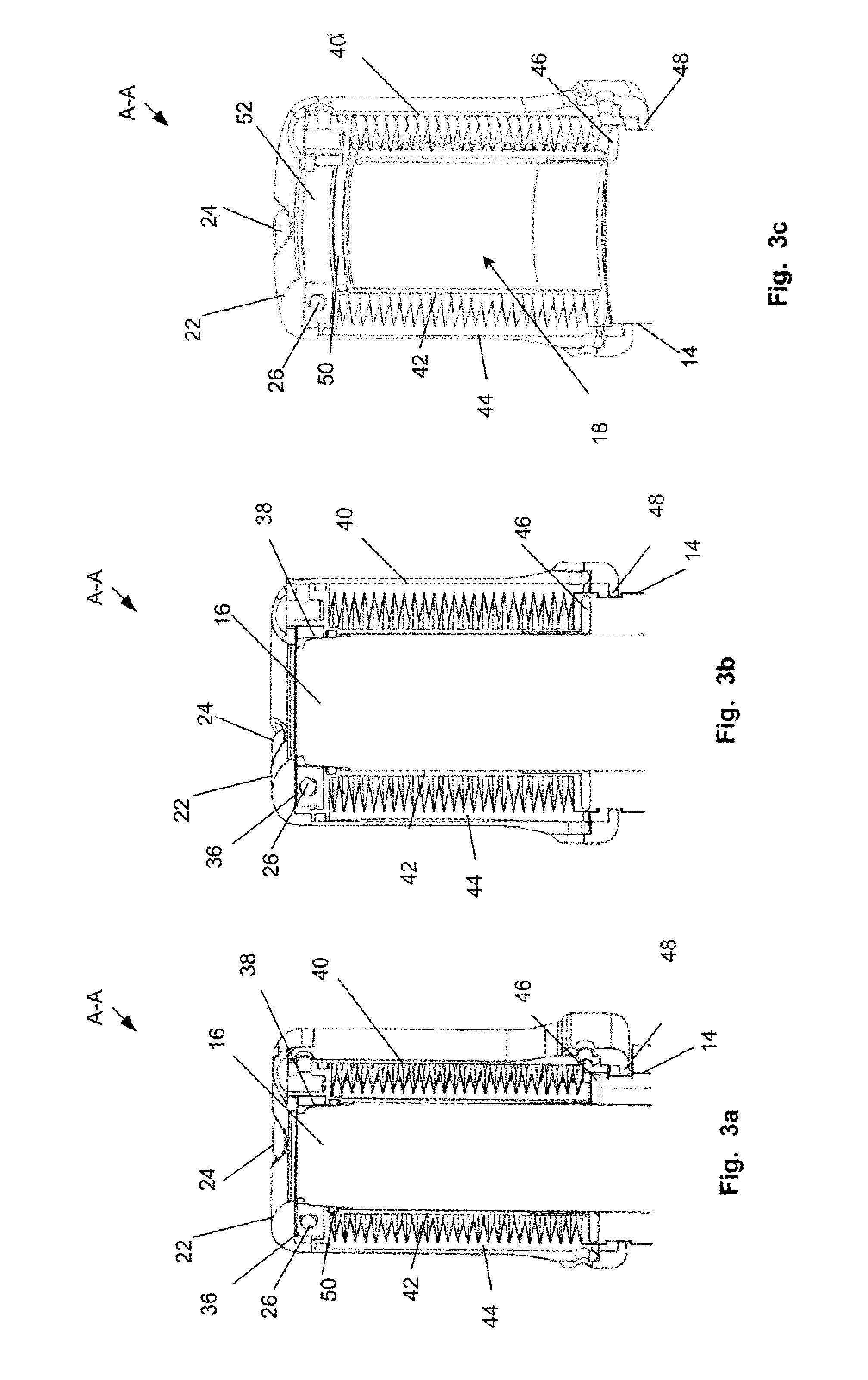
[0113]The biological navigation device 10 can have a head 12, a tube 14 or a combination thereof. The head 12 can hav...
PUM
 Login to View More
Login to View More Abstract
Description
Claims
Application Information
 Login to View More
Login to View More - R&D
- Intellectual Property
- Life Sciences
- Materials
- Tech Scout
- Unparalleled Data Quality
- Higher Quality Content
- 60% Fewer Hallucinations
Browse by: Latest US Patents, China's latest patents, Technical Efficacy Thesaurus, Application Domain, Technology Topic, Popular Technical Reports.
© 2025 PatSnap. All rights reserved.Legal|Privacy policy|Modern Slavery Act Transparency Statement|Sitemap|About US| Contact US: help@patsnap.com